You were doing everything right. The medication was working. The scale was moving. You felt it — the momentum, the clothes fitting differently, the hope that this time was going to be different.
And then… nothing.
The scale stopped. You didn’t change anything. You’re still taking your medication, still watching what you eat, still trying — but the number won’t budge. Welcome to the weight loss plateau. And after 50, it hits harder, lasts longer, and takes a smarter strategy to break.
This isn’t a failure of willpower. It’s biology. Here’s what’s actually happening — and what you can do about it.
Why Plateaus Happen After 50
Your body after 50 is operating on a completely different set of rules than it did in your 30s. Several things converge at once:
Hormonal shifts change everything. Estrogen and progesterone decline during menopause, and this directly impacts how and where your body stores fat — especially around the abdomen. Lower estrogen also reduces insulin sensitivity, making it harder for your cells to process glucose efficiently. The result? Your body gets better at holding onto fat as a survival strategy.
Your metabolism adapts to your new lower calorie intake. When you eat less — which GLP-1 medications make easier by suppressing appetite — your body gets the memo and adjusts its metabolic rate downward. It’s called adaptive thermogenesis, and it’s one of the main reasons the scale stops moving even when you’re doing everything right. Your body becomes more efficient at running on less fuel.
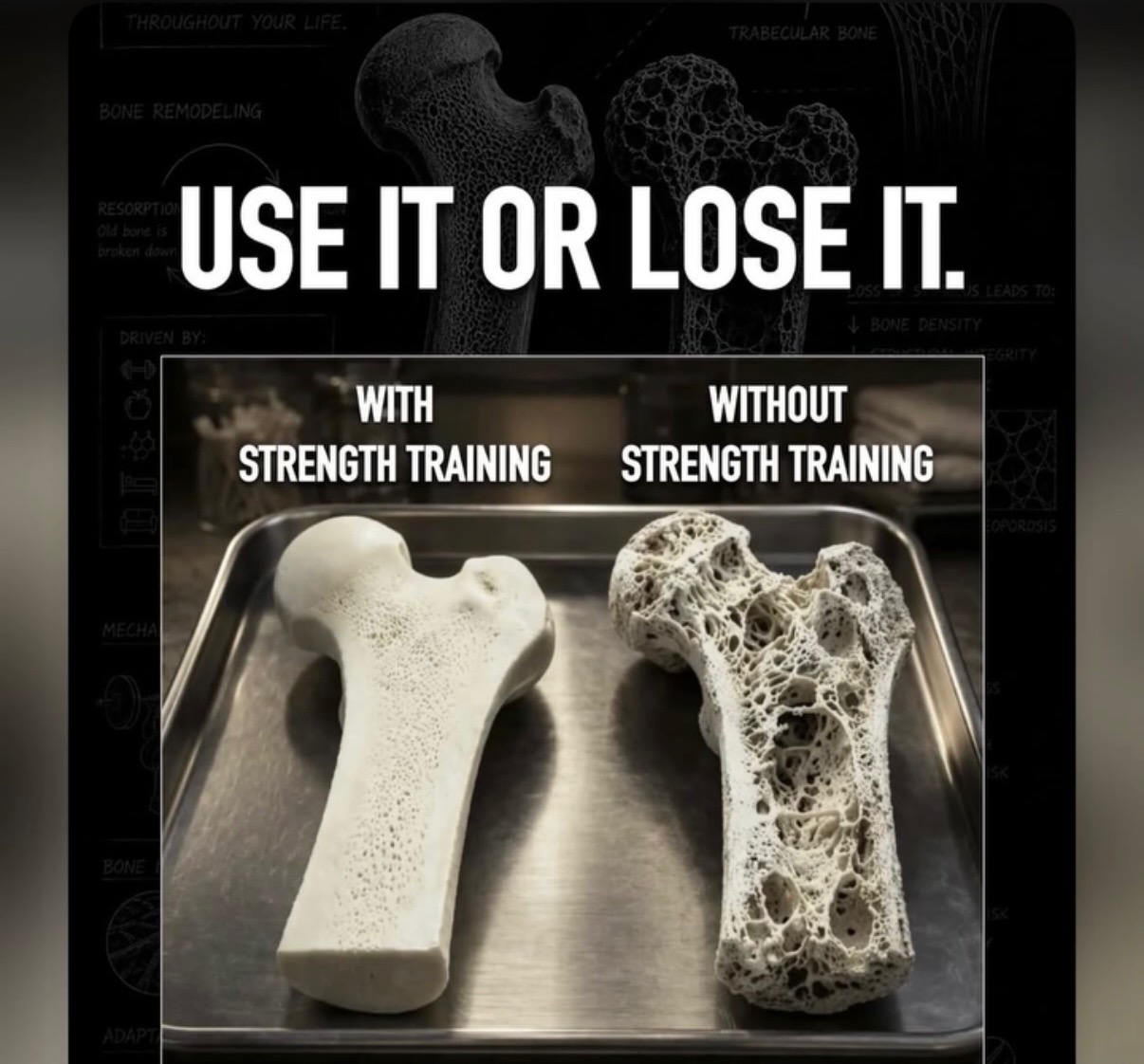
Muscle mass declines with age. After 40, women lose about 3-8% of their muscle mass per decade without active intervention. Muscle is metabolically expensive — it burns calories even at rest. Less muscle means a slower resting metabolic rate. And if your GLP-1 program isn’t prioritizing muscle preservation, you may be losing muscle alongside fat, making the plateau worse over time.
Cortisol and stress become bigger players. Chronic stress elevates cortisol, which signals your body to hold onto belly fat as an energy reserve. After 50, sleep disruptions, life transitions, and the mental load of weight loss itself can all spike cortisol — working directly against your progress.
The Biggest Mistakes Women Make on GLP-1 Programs
GLP-1 medications like Semaglutide and Tirzepatide are powerful tools. But a tool is only as good as the strategy around it. Here are the most common mistakes I see that stall results:
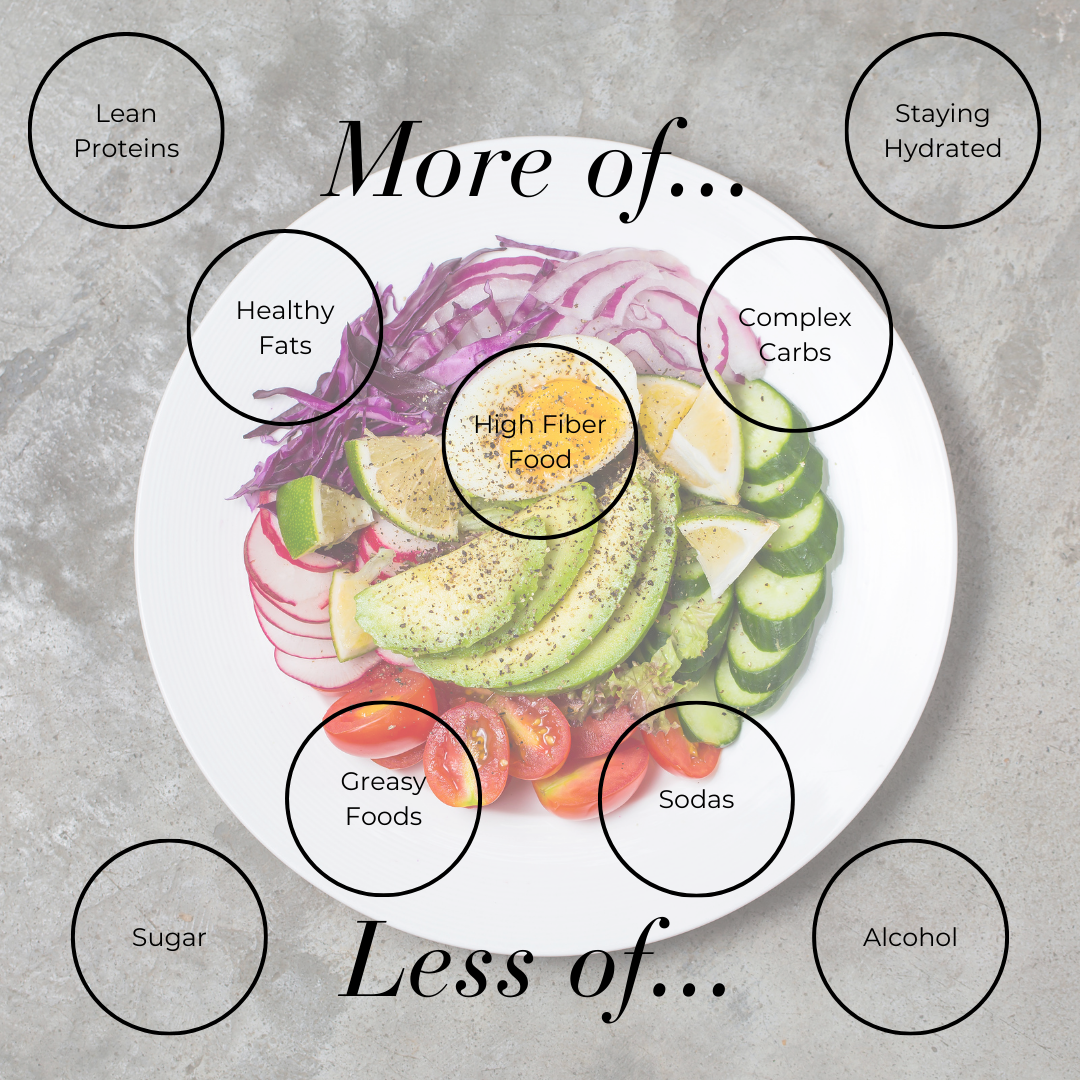
Eating too little protein. GLP-1 medications suppress appetite significantly — sometimes to the point where clients are barely eating. When you don’t eat enough protein while in a calorie deficit, your body breaks down muscle for energy. Less muscle = slower metabolism = harder plateau to break. Most women on GLP-1s need at least 100-120g of protein per day, and many are getting half that.
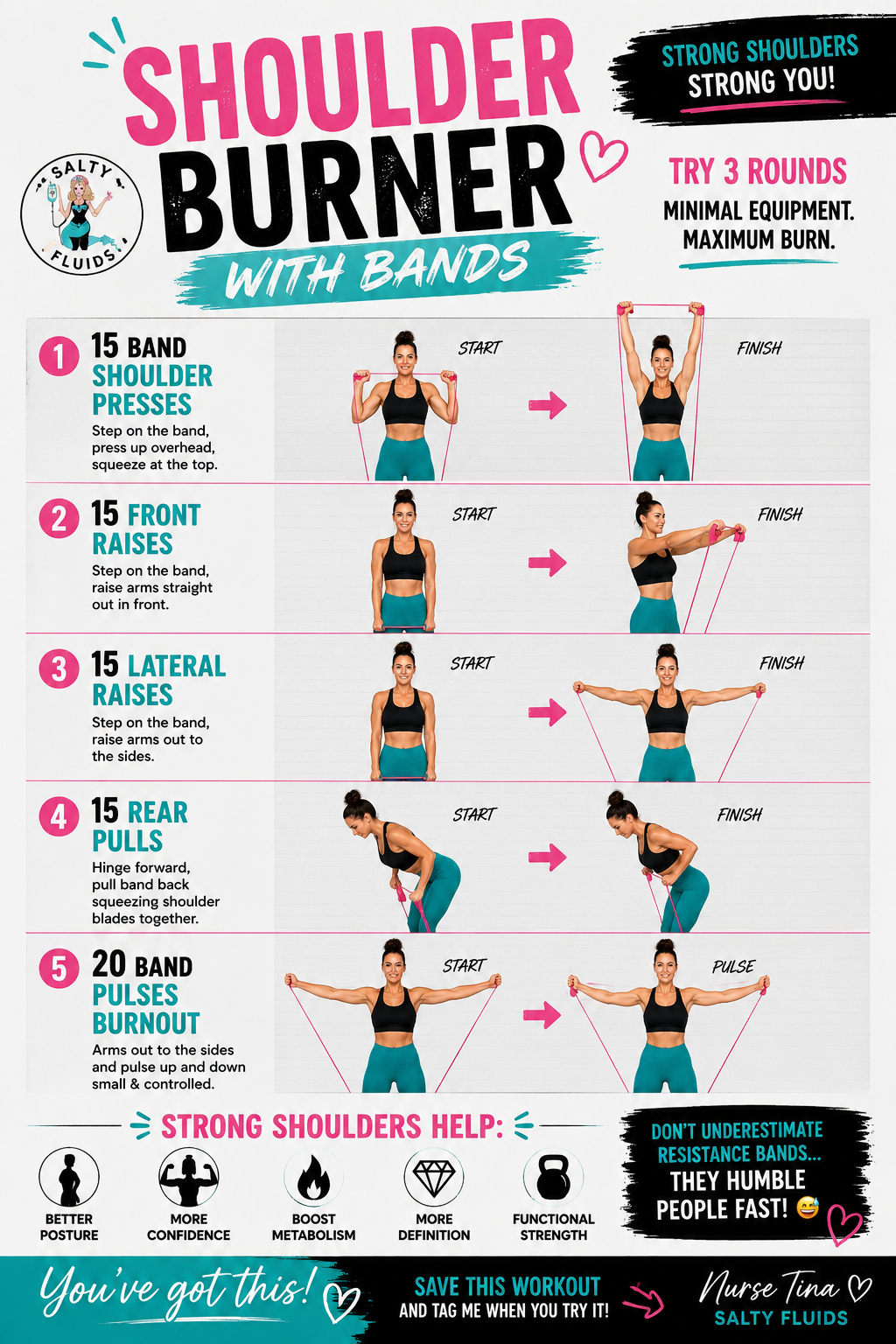
Not strength training. Cardio burns calories in the moment. Strength training rebuilds metabolic tissue — muscle — that burns calories around the clock. If you’re only doing cardio, you’re missing the most powerful long-term fat-loss lever available to you. Even two sessions per week of resistance training can significantly shift your body composition and metabolic rate.
Not drinking enough water — or the wrong kind. Dehydration slows metabolism, increases hunger signals, and can make fatigue feel like a plateau. On GLP-1 medications, nausea can make drinking feel hard. But staying hydrated is non-negotiable. If drinking water is a struggle, IV hydration can bypass the stomach entirely and restore your cells’ fluid and electrolyte balance directly.
Expecting the medication to do all the work. GLP-1 medications reduce appetite. They do not optimize nutrition, rebuild muscle, balance hormones, or improve sleep. The medication creates the window — what you do inside that window determines your long-term outcome.
Inconsistent injection timing. Semaglutide and Tirzepatide need consistency to maintain stable blood levels. Injecting even a day or two late can create appetite fluctuations that lead to overeating and undo your progress. Set a reminder. Same day, same time, every week.
Skipping sleep. During deep sleep, your body releases growth hormone — the primary driver of fat metabolism and muscle repair. Poor sleep spikes ghrelin (the hunger hormone) and drops leptin (the fullness hormone), making it biochemically harder to eat less the next day. If you’re sleeping fewer than 7 hours, your weight loss is working against a significant headwind.
7 Ways to Break a Weight Loss Plateau After 50
Plateaus are not permanent — but they do require strategy. Here’s what actually moves the needle:
1. Audit your protein. Download a food tracking app for one week and log everything. Most women discover they’re eating 50-70g of protein when they need 100-130g. Prioritize protein at every meal — especially breakfast. Aim for 30-40g before noon to front-load muscle-protecting amino acids while your body is most anabolic.
2. Add resistance training (or increase it). You don’t need a gym. Bodyweight exercises, resistance bands, or free weights 2-3 times per week can begin to rebuild metabolic tissue within weeks. Focus on compound movements: squats, deadlifts, rows, presses. These recruit the most muscle and produce the highest metabolic response.
3. Reverse diet for 2-3 weeks. Counterintuitive but effective: if you’ve been in a deep calorie deficit for months, try adding 100-200 calories per day for 2-3 weeks. This signals your body that starvation mode is over, nudges metabolic rate upward, and often triggers a new round of fat loss when you return to your deficit.
4. Prioritize sleep like a job. Set a sleep window and protect it. No screens after 9 PM. Keep your room cool and dark. Magnesium glycinate before bed supports deeper sleep and reduces cortisol. If sleep is chronically disrupted, address it — everything else becomes less effective when sleep is broken.
5. Address stress directly. Chronic elevated cortisol is one of the most under-addressed weight loss blockers for women over 50. Breathwork, walking in nature, prayer, journaling — whatever genuinely lowers your nervous system activation. This isn’t optional self-care fluff. It’s a metabolic intervention.
6. Refocus on body composition, not just weight. If you’re gaining muscle while losing fat, the scale may not move — but your body is transforming. Take measurements, notice how clothes fit, track energy levels. The scale is one data point. It is not the full picture.
7. Support your cells with IV hydration. When appetite suppression is high and nutrition is compromised, your cells can be running on empty without obvious hunger signals to warn you. IV hydration delivers fluids, electrolytes, and optional nutrient add-ons directly into your bloodstream — bypassing a sensitive stomach entirely. Clients on GLP-1 programs often feel a significant energy and clarity shift after an IV session, which makes it easier to exercise, eat intentionally, and stay consistent.
The Bottom Line
A plateau is your body’s way of asking for more support — not a sign that you should give up. After 50, weight loss requires a more sophisticated strategy than simply eating less and moving more. It requires protecting muscle, optimizing sleep, managing stress, staying hydrated, and giving your body the right inputs at the cellular level.
GLP-1 medications are one of the most powerful tools available for breaking through biological resistance to weight loss. But they work best as part of a nurse-led plan that accounts for all the variables — not just appetite suppression.
If you’ve hit a wall, you don’t have to figure it out alone. Book a free 15-minute consult and let’s look at what’s actually going on — and build a plan to get you moving again.
Tina Yakel, RN
Salty Fluids
“Feel like yourself again… but hotter.”